The Schroth Method
Katharina Schroth
What is the
Schroth Method?
The Schroth Method is a conservative exercise approach to the treatment of scoliosis and postural dysfunction. The Schroth Method teaches 3-D correction of the spine, and is part of a class of exercises referred to as PSSE (Physiotherapy Scoliosis Specific Exercises).
The Schroth Method is one part of a multidisciplinary, collaborative approach to the conservative management of scoliosis. The exercises within the Schroth Method are performed in a variety of positions, each highlighting how muscles work against gravity in that specific position to open trunk concavities and promote de-rotation and deflection of the scoliosis. Every person is unique and exercises are determined based on individual curve patterns, physical ability, age, and other factors.
Find out moreWhat’s the story with the Body Blocks?
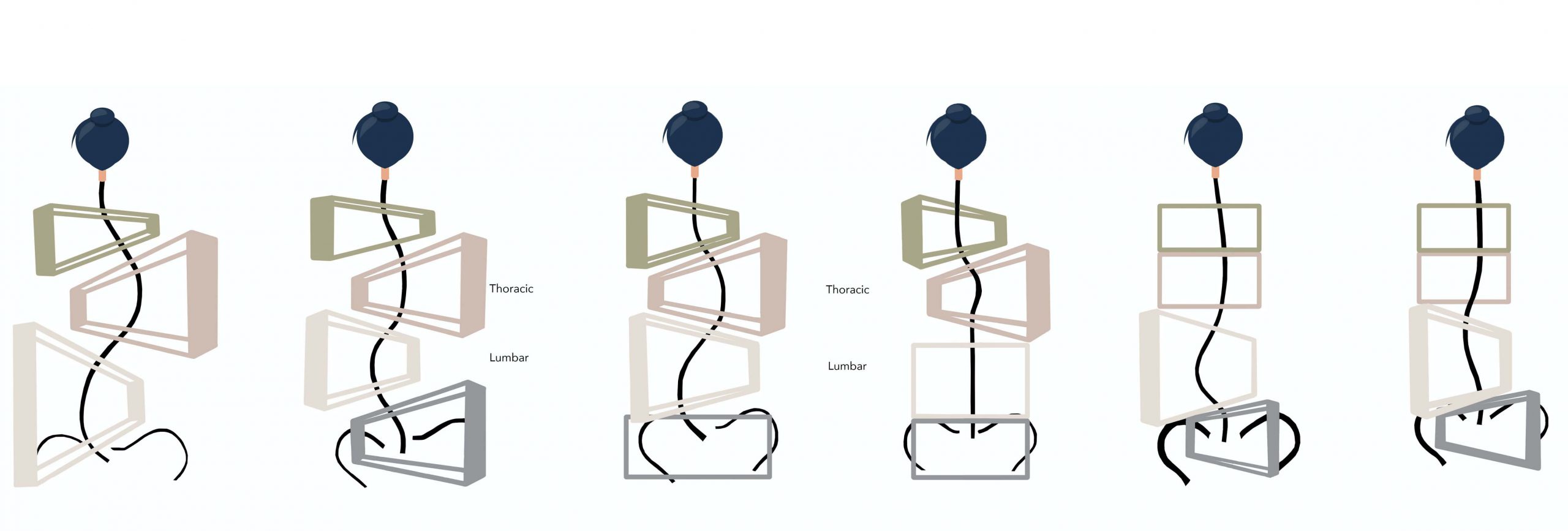
The blocks are shifted and rotated to represent the regions of the spine (cervical, thoracic, lumbar and sacrum / pelvis) that are laterally, posteriorly and anteriorly rotated with respect to one’s curve pattern. The smaller side of the block represents the concave side of a curve, and the wider (and taller) side of the block represents the convex side of a curve.
About Scoliosis
Scoliosis is a complex three-dimensional phenomena involving vertebral wedging, extension, and rotation that transforms the entire shape of the trunk and its ability to optimally transfer forces during movement. Scoliosis can be screened clinically by having the individual perform an Adam’s Forward Bend Test, but is confirmed radiologically on X-ray with a Cobb Angle > 10º.
Functional scoliosis is the spine’s attempt to upright and level the head and eyes to compensate for muscular imbalances. In this type of scoliosis, an Adam’s Forward Bend Test is negative, with no visible rib hump or asymmetry. Over time, though, a functional scoliosis can become structural.
Structural scoliosis involves lateral wedging and rotation of both the discs and the vertebrae and impacts the entire 3D shape of the spine, rib cage and torso. In a structural scoliosis, the Adam’s Forward Bend Test is positive, revealing a visible rib hump in one or more areas of the back. In a structural scoliosis, not only are the vertebrae laterally shifted and rotated, but the shoulders, rib cage, and pelvic blocks are, too.
- affects 3-4% of the population
- affects females and males equally, but females have 8x risk for curve progression to levels that require treatment.
- can develop at various stages of life, but most commonly presents during adolescence
- tends to progress during periods of rapid growth for both males and females, and peri-menopause in females
- Idiopathic (no known cause or etiology) 75-80%
- De Novo (adult onset with no known history, also known as degenerative scoliosis)
- Neuromuscular (5-7%)
- Congenital (10%)
- Other (secondary to other conditions, including Marfan’s syndrome, tumors, etc)
The current working definition of idiopathic scoliosis is: “A complex 3D torsional deformity of the spine and the trunk (CE Aubin) which appears in apparently healthy children, and can progress in relation to multiple factors during any rapid period of growth or later in life.”
Source: M Rigo, MD; Th Grivas, MD; J O’Brien, Scoliosis (2010)
- Idiopathic Scoliosis is classified according to the age of onset, not necessarily the age of diagnosis.
- Infantile Idiopathic Scoliosis (IIS) 0-3 years old
- Juvenile (Idiopathic Scoliosis JIS) 4-10 years old
- Adolescent Idiopathic Scoliosis (AIS) 11-18 years old
- Adult Scoliosis
a) Adolescent scoliosis that continues into adulthood
b) DeNovo – adult onset with no previously known history of scoliosis
Many factors can contribute to the development of scoliosis, including genetics, biomechanics, low levels of Vitamin D, calcium, magnesium, leptin, the presence of osteoporosis or osteopenia, and more.
In Idiopathic Scoliosis (IS), while there is no known cause yet, many theories exist, but the most current scientifically accepted theory is the Bi-NOTOM (double neuro-osseous timing of maturation) theory proposed in 2009 by RG Burwell et al in Scoliosis.
Congenital Scoliosis initiates in utero due to malformation of one or more vertebrae or during gestation. Although the skeletal asymmetry is present at birth, congenital scoliosis may not progress or become evident until later stages of growth in childhood or adolescence.
Neuromuscular Scoliosis involves asymmetry of the spine secondary to neuromuscular diagnoses such as cerebral palsy (CP), muscular dystrophy (MD), spinal muscular atrophy (SMA), and more. The nature, presentation, and treatment of neuromuscular scoliosis is quite different from Idiopathic Scoliosis
Adult Onset/Degenerative, or De Novo Scoliosis is a scoliosis that develops in adulthood (usually > age 40) and is secondary to osteopenia, osteoporosis, muscle weakness, postural imbalances and chronic asymmetric loading of the disc and spinal facet joints. This type of scoliosis is most common in the lower thoracic and lumbar spine due to the foundational nature and most loaded region of the vertebral column.
- Possible trunk imbalance/leaning to the right or left side
- Possible pelvic shift to the right or left side, opposite the primary curve.
- One shoulder higher/lower than the other
- Asymmetric rotation in shoulders
- Uneven shoulder blades
- Uneven waistline
- One hip possibly elevated
- Visible prominence (rib hump) observed from behind during a forward bend or spinal flexion
- Spinous processes not in a straight line (non-rectilinear)
While postural asymmetries such as scoliosis and hyperkyphosis (Scheuermann’s Kyphosis) are screened for clinically, radiographic imaging such as X-rays or MRI are required to confirm a diagnosis. EOS X-rays are a great option that many families choose to explore, as EOS provides a beautiful full-spine image at often a fraction of the radiation exposure of traditional X-rays.
Many treatment options exist to support individuals and families with scoliosis.
- Observation
- Physiotherapeutic Scoliosis Specific Exercise (PSSE)
- Bracing
- Surgery
Physiotherapeutic Scoliosis Specific Exercise (PSSE) differs from traditional physical therapy on many levels and is truly a specialized field requiring extensive training and certification post graduate school. While there are a number of PSSE methods globally, the standard features of all PSSE programs are to:
- optimize 3-dimensional postural balance
- promote neutral spine core stability to so that the new, midline and balanced posture becomes the individual’s new habitual postural.
- educate and train patients on optimal body mechanics with activities of daily living (ADLs)
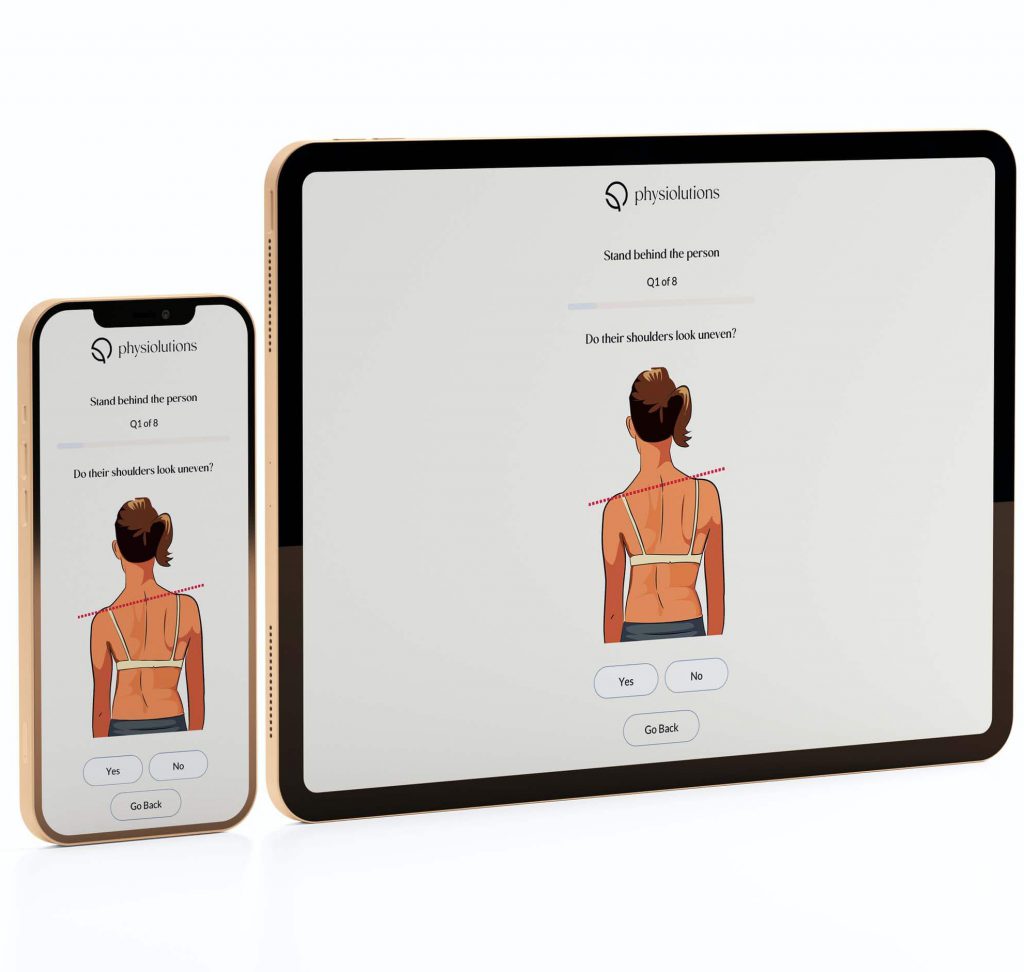
Clarity App™
Self Screen for Scoliosis
Scoliosis is a complex three-dimensional phenomena involving vertebral wedging, extension, and rotation that transforms the entire shape of the trunk and its ability to optimally transfer forces during movement. Scoliosis can be screened clinically by having the individual perform an Adam’s Forward Bend Test, but is confirmed radiologically on X-ray with a Cobb Angle > 10º.